What Is Fever?
Fever is one of the most common symptoms experienced by people of all ages, yet it remains widely misunderstood. Often perceived as an illness itself, fever is, in reality, a vital sign—a physiological response orchestrated by the body to signal that something is amiss. It serves as both a defense mechanism and a call to action, prompting individuals to seek rest, hydration, and, when necessary, medical attention.

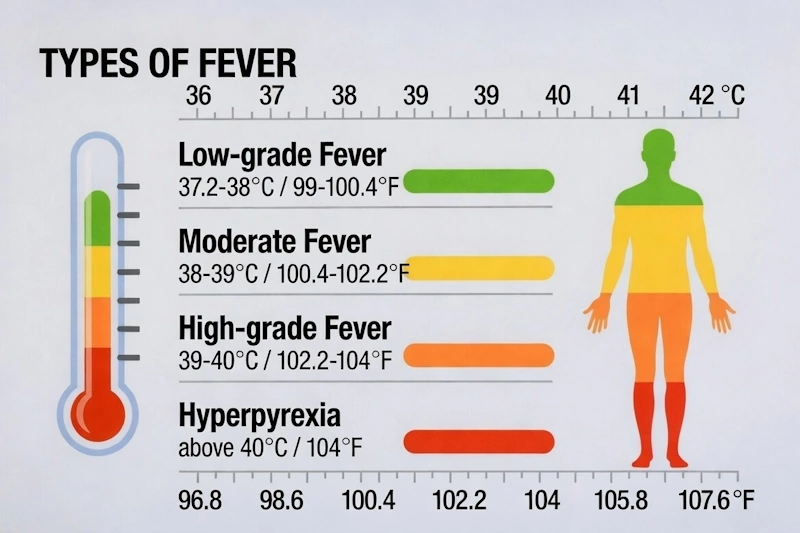
At its core, fever is defined as a temporary elevation in body temperature, typically above 38°C (100.4°F) when measured orally. This rise in temperature is not random; it is a carefully regulated process initiated by the immune system in response to infection, inflammation, or other underlying conditions.
Fever can occur in a variety of contexts. Infections, such as those caused by bacteria, viruses, or fungi, are the most common triggers. However, non-infectious causes, including autoimmune diseases, certain medications, heat exhaustion, and even cancers, can also induce a febrile response. The timing and pattern of fever—whether it spikes suddenly, lingers for days, or recurs intermittently—can provide valuable clues to its underlying cause.
How fever occurs?
When our body encounters something potentially harmful, like bacteria or viruses, a complex chain of events begins. Think of it like setting off a sophisticated alarm system in your house, but instead of sound, it produces heat.
First, our immune cells detect what we call “pyrogens.” These can come from two sources: either from outside our body (like bacterial toxins) or from inside (produced by our own immune cells). These pyrogens act as messengers, traveling through our bloodstream until they reach a special control center in our brain called the hypothalamus.
The hypothalamus works like our body’s thermostat. Normally, it keeps our body temperature around 37°C (98.6°F). However, when pyrogens arrive, they trigger the production of a substance called prostaglandin E2. This substance essentially “resets” our body’s thermostat to a higher temperature.
These pyrogens can be exogenous (from outside the body, such as bacterial toxins) or endogenous (produced by the body’s own cells, particularly cytokines like interleukin-1 and tumor necrosis factor). The resulting fever serves several immunological advantages: it enhances immune cell function, creates an unfavorable environment for many pathogens, and accelerates tissue repair processes.
Once the thermostat is reset, our body starts several processes to increase its temperature:
- Muscles begin to contract rapidly, creating heat (this is why we shiver)
- Our metabolism speeds up, generating more heat
- We might feel cold and seek warmth (like grabbing a blanket)
As these processes continue, our body temperature rises until it reaches the new, higher setpoint. This elevated temperature actually helps our body fight infection in several ways. It speeds up our immune system’s response, makes it harder for many bacteria and viruses to multiply, and accelerates our body’s repair processes.
When the infection or threat begins to clear, our body produces anti-inflammatory substances that gradually reset the hypothalamus back to its normal temperature setting. This is when we start feeling hot and sweating as our body works to cool back down to its usual temperature.
Classification of fever patterns
Medical professionals recognize several distinct fever patterns, each potentially indicating different underlying conditions:
- Continuous fever maintains an elevated temperature with minimal fluctuation (less than 1°C variation), often seen in lobar pneumonia or typhoid.
- Intermittent fever shows normal temperature periods alternating with fever spikes, common in malaria and sepsis.
- Remittent fever fluctuates daily but never returns to normal, characteristic of various viral infections.
- Hectic fever presents large daily fluctuations, often associated with severe infections or malignancies.
Clinical assessment
When evaluating fever, medical practitioners consider multiple factors beyond just temperature measurement. The pattern and timing of temperature elevation, associated symptoms, recent travel history, medication use, and underlying medical conditions all contribute to the diagnostic process. The presence of accompanying signs like rigors (severe shaking), sweating, or specific pain locations helps narrow down potential causes.
Temperature measurement methods vary in accuracy and appropriateness for different situations. While rectal temperature provides the most accurate core reading, oral and tympanic measurements offer practical alternatives in most clinical settings.
Medical professionals must look for following conditions, symptoms and status:
- Infections
- Non-infectious inflammations, such as autoimmune diseases
- Malignancies
- Medications
- Endocrine disorders
- Thromboembolic disease
- Factitious fever
- Travel history?
- Geographic upbringing?
- Family history?
- Occupation?
- Substance abuse?
- Infants in the household?
- Illnesses in the surrounding environment?
- Past illnesses, especially heart disease or autoimmune disease?
- Foreign body materials?
- Medications?
- Joint pain?
- Tachycardia?
- Weight loss?
- Night sweats?
- Focal symptoms? Runny nose? Cough? UTI symptoms? Diarrhea?
Status
- Does the patient actually have a fever?
- Oral cavity and throat normal? Pressure-sensitive teeth?
- Tenderness over the sinuses?
- Tenderness over the temporal artery?
- Heart murmur? Tachycardia?
- Normal lung auscultation?
- Lymph nodes? Resistance or tenderness in the abdomen?
- Tenderness over the thyroid?
- Tenderness on percussion over the kidney areas?
- Prostate tenderness? Normal rectal palpation?
- Skin changes? Redness in the nail beds?
- Joint swelling?
- Bone tenderness?
- Neurologically normal? Tremor?
Diagnostic approach
The diagnostic workup for fever follows a systematic approach. Initial evaluation includes detailed history taking and physical examination. Laboratory investigations typically begin with complete blood count, comprehensive metabolic panel, blood cultures, and urinalysis. Additional tests such as chest X-rays, inflammatory markers (ESR, CRP), or specific disease markers may be ordered based on clinical presentation.
Basic Investigation:
- Blood cultures
- Urine cultures
- Erythrocyte sedimentation rate (ESR)
- C-reactive protein (CRP)
- White blood cell count (WBC)
- Differential white cell count
- Platelet count (PLT)
- Aspartate transaminase (AST/ASAT)
- Alanine transaminase (ALT/ALAT)
- Alkaline phosphatase (ALP)
- Bilirubin
- Sodium
- Potassium
- Creatinine
- Calcium
- Serum protein electrophoresis (SPEP)
- Serum lactate dehydrogenase (LDH/S-LD)
- Thyroid-stimulating hormone (TSH) / Free T4
- Urine dipstick test
- Chest X-ray
Extended or supplementary investigations that may be relevant depending on medical history, symptoms, findings on examination, and results of the above laboratory tests:
- CMV serology
- EBV serology
- Monospot test
- Thyroid function tests
- Temporal artery biopsy
- ANA (antinuclear antibody)
- Rheumatoid factor
- ANCA (antineutrophil cytoplasmic antibodies)
- CT scan of the abdomen
- Ultrasound of the liver and gallbladder
- Transesophageal echocardiogram
- PPD (tuberculin skin test)
- Gynecological examination
- Liver biopsy
- Bone marrow examination
- HIV antibodies
- Wasserman test (WR)
- Fecal occult blood (F-Hb)
- Serum uric acid (S-Urate)
- Angiotensin-converting enzyme (ACE)
- Malaria smear
- Mycobacterium cultures
- TNF receptor 1
- PET scan
Complications and special considerations
Extreme elevation in body temperature (hyperpyrexia, typically above 41.5°C or 106.7°F) can lead to serious complications including delirium, seizures, and organ damage. Certain patient populations require special attention: young children may experience febrile seizures, while elderly patients might not mount significant fever despite serious infection.
Neuroleptic malignant syndrome, malignant hyperthermia, and heat-related illnesses represent important differential diagnoses where elevated temperature occurs through mechanisms distinct from the typical fever pathway.
Infections
- Infective Endocarditis
- Listen for heart murmurs! Blood cultures are crucial. CRP and ESR can often be close to normal levels.
- Deep Abscesses (e.g., Liver and Lung Abscesses)
- Common in patients with poor general health or alcohol-related issues. Can sometimes mimic malignancy with gradual weight loss and low-grade fever.
- Osteomyelitis and Septic Arthritis
- Often present with focal symptoms from the affected area.
- Cytomegalovirus (CMV)
- Often seen in previously seronegative new fathers or grandparents infected via diaper changes from asymptomatic viral shedding in a child’s urine. Elevated transaminases. Positive IgM CMV.
- Mononucleosis (Glandular Fever)
- Can occur in a septic form without visible lymph node enlargement or throat symptoms. Diagnosed via Monospot, blood work, and potentially serology.
- Tuberculosis (TB)
- Primarily seen in immigrants (especially from Africa and Asia) and older Swedish individuals. Cultures from symptomatic sites and histopathological examination of lymph nodes confirm the diagnosis. Chest X-ray recommended.
Non-infectious auto-inflammatory and autoimmune diseases
- Temporal Arteritis, Giant Cell Arteritis (GCA), and Polymyalgia Rheumatica (PMR)
- Pain and stiffness in large muscle groups, especially in the morning. Elevated ESR, CRP, ALP, and platelet count. Temporal artery biopsy can confirm the diagnosis in temporal arteritis. Rapid and dramatic improvement is expected after initiating corticosteroids per treatment guidelines.
- Systemic Lupus Erythematosus (SLE)
- Often involves multiple organs, sometimes with butterfly-shaped rash.
- Granulomatosis with Polyangiitis (Wegener’s Granulomatosis)
- Often presents with lung symptoms or sinus involvement.
- Adult-Onset Still’s Disease
- Skin changes, often conjunctivitis, neutrophilia.
- Sweet’s Syndrome (Febrile Neutrophilic Dermatosis)
- Tender skin lesions.
- Tumor Necrosis Factor Receptor-Associated Periodic Syndrome (TRAPS)
- Very rare. Often presents with myalgia, peritonitis, and intermittent fever.
- Periodic Fever with Aphthous Stomatitis, Pharyngitis, and Cervical Adenitis (PFAPA)
- A cause of fever in children.
- Familial Mediterranean Fever
- Often presents with myalgia, peritonitis, and intermittent fever.
- Sarcoidosis
- Often involves extrapulmonary manifestations in cases of unexplained fever.
- Gout
- Commonly involves an inflamed big toe joint but can also affect other joints and organs. Elevated serum uric acid (S-Urate) is typically observed.
Malignancies
Malignant fever almost always has an inflammatory component (e.g., elevated ESR, haptoglobin, and platelet count), and S-LD is usually elevated as a sign of cell destruction.
- Hodgkin’s lymphoma
- Non-Hodgkin’s lymphoma
- Leukemia
- Renal cell carcinoma (hypernephroma)
- Multiple myeloma (myelomatosis)
- Ovarian cancer
- Lung cancer
Medications
Many medications can cause fever. The most common are:
- Angiotensin II receptor blockers
- ACE inhibitors
- Phenytoin
- Lamotrigine
- Rifampicin
- Hydralazine (Apresoline)
- Nitrofurantoin (Furadantin)
- Prolonged treatment with beta-lactam antibiotics
- Chemotherapy drugs (cytostatics)
- Interferon
- Antipsychotics (neuroleptics)
Endocrine diseases
- Hyperthyroidism
Often associated with tachycardia, weight loss, and diarrhea. In subacute thyroiditis (de Quervain), there may be pain during swallowing and tenderness on palpation of the thyroid gland.
Thromboembolic disease
- Chronic Pulmonary Embolism
Often presents with dyspnea.
Factitious fever
Self-induced fever is rare. Young, single women in healthcare-related professions are overrepresented. Blood cultures or cultures from abscesses may sometimes test positive for unusual mixed flora. Fever in children can sometimes be caused by parental behavior.
Treatment
Medical treatment
When doctors treat fever, they focus on two aspects: addressing the underlying cause and managing the symptoms. The choice of treatment depends on what’s causing the fever and how severe it is.
For bacterial infections, doctors prescribe appropriate antibiotics based on the likely causative organism or culture results. Viral infections generally don’t require specific medication since viruses typically resolve on their own, but certain cases might need antiviral medications.
The main medications used to reduce fever (antipyretics) include:
- Acetaminophen (Tylenol) works by affecting the temperature control center in the brain. It’s generally considered safe and effective, but doctors carefully monitor the daily dose to prevent liver damage.
- NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) like ibuprofen or naproxen not only reduce fever but also decrease inflammation. They work by blocking prostaglandin production, which helps reset the body’s temperature threshold. However, these medications require careful use as they can affect kidney function and stomach lining.
Home treatment
Home care plays a crucial role in managing fever and supporting recovery. Here’s how you can effectively manage fever at home:
- Hydration is absolutely essential. Fever increases fluid loss through sweating and faster breathing, so drinking plenty of water, clear broths, or electrolyte solutions helps prevent dehydration. Room temperature fluids often work better than very cold ones.
- Keep cool. Keeping room temperature comfortable (around 70-74°F/21-23°C) and wearing light clothing allows proper heat release. A lukewarm bath or compress might help, but never use cold water as it can cause shivering and actually raise body temperature.
- Take a rest. Your body needs extra energy to fight infection. Limiting physical activity and getting adequate sleep supports the immune system’s work.
- Eat well. Proper nutrition, even if appetite is reduced, helps maintain strength. Light, easily digestible foods are usually best. If eating is difficult, liquid nutrition like broths or smoothies can help maintain energy levels.
When to seek medical care?
Understanding when to move beyond home treatment is crucial. Contact healthcare providers if:
- Temperature exceeds 103°F (39.4°C) in adults
- Fever lasts more than three days
- Severe headache or neck stiffness develops
- Confusion or excessive sleepiness occurs
- Difficulty breathing arises
- Signs of dehydration appear despite fluid intake
- New or severe symptoms develop
Different age groups require different approaches. Infants and elderly individuals need more careful monitoring and often lower thresholds for seeking medical care. People with certain medical conditions or taking specific medications might need modified treatment approaches.
Sources & References
- Axelrod, P. (1990) ‘External cooling in the management of fever’, Clinical Infectious Diseases, 12(Suppl 5), pp. S582–S590. Available at: https://pubmed.ncbi.nlm.nih.gov/2190795/
- Avner, J.R. (2009) ‘Acute fever’, Pediatric Clinics of North America, 56(2), pp. 387–413. Available at: https://pubmed.ncbi.nlm.nih.gov/19393943/
- Barbi, E. et al. (2017) ‘Fever in children: pearls and pitfalls’, Children (Basel), 4(9), p. 81. Available at: https://pubmed.ncbi.nlm.nih.gov/28925980/
- Bleeker-Rovers, C.P. et al. (2007) ‘Fever of unknown origin’, Clinical Medicine (London), 7(2), pp. 136–140. Available at: https://pubmed.ncbi.nlm.nih.gov/17512471/
- Chiappini, E. et al. (2017) ‘Fever management: a European expert panel perspective’, European Journal of Pediatrics, 176(7), pp. 955–963. Available at: https://pubmed.ncbi.nlm.nih.gov/28536848/
- Cunha, B.A., Lortholary, O. and Cunha, C.B. (2015) ‘Fever of unknown origin: a clinical approach’, American Journal of Medicine, 128(10), pp. 1138.e1–1138.e15. Available at: https://pubmed.ncbi.nlm.nih.gov/26093175/
- Dinarello, C.A. (2004) ‘Infection, fever, and exogenous and endogenous pyrogens: some concepts have changed’, Journal of Endotoxin Research, 10(4), pp. 201–222. Available at: https://pubmed.ncbi.nlm.nih.gov/15321145/
- Hayakawa, K. et al. (2012) ‘Fever of unknown origin: an evidence-based review’, American Journal of Medical Science, 343(1), pp. 57–64. Available at: https://pubmed.ncbi.nlm.nih.gov/21881409/
- Knockaert, D.C., Vanneste, L.J. and Bobbaers, H.J. (1993) ‘Fever of unknown origin in the 1980s. An update of the diagnostic spectrum’, Archives of Internal Medicine, 153(13), pp. 1541–1549. Available at: https://pubmed.ncbi.nlm.nih.gov/8325521/
- Mackowiak, P.A. (1994) ‘Fever: blessing or curse? A unifying hypothesis’, Annals of Internal Medicine, 120(4), pp. 310–316. Available at: https://pubmed.ncbi.nlm.nih.gov/8267655/
- Marik, P.E. (2010) ‘Fever in the ICU’, Chest, 138(4), pp. 974–980. Available at: https://pubmed.ncbi.nlm.nih.gov/20923898/
- Netea, M.G. et al. (2020) ‘Defining trained immunity and its role in periodic fever syndromes’, Cell Host & Microbe, 28(2), pp. 169–175. Available at: https://pubmed.ncbi.nlm.nih.gov/32783972/
- Niven, D.J. et al. (2012) ‘Fever in hospitalized medical patients: characteristics and significance’, Journal of Critical Care, 27(6), pp. 741.e9–741.e16. Available at: https://pubmed.ncbi.nlm.nih.gov/22503313/
- Ogoina, D. (2011) ‘Fever, fever patterns and diseases called ‘fever’ – A review’, Journal of Infection and Public Health, 4(3), pp. 108–124. Available at: https://pubmed.ncbi.nlm.nih.gov/22985727/
- Sorensen, H.T. et al. (2014) ‘Fever and the risk of cardiovascular events’, European Heart Journal, 35(47), pp. 3267–3275. Available at: https://pubmed.ncbi.nlm.nih.gov/25070001/
- Sullivan, J.E. and Farrar, H.C. (2011) ‘Fever and antipyretic use in children’, Pediatrics, 127(3), pp. 580–587. Available at: https://pubmed.ncbi.nlm.nih.gov/21357344/
- Sundén-Cullberg, J., Rantell, J. and Lipworth, L. (2017) ‘Fever in the critically ill medical patient’, American Journal of Respiratory and Critical Care Medicine, 196(3), pp. 293–300. Available at: https://pubmed.ncbi.nlm.nih.gov/28248508/
- Unger, M. et al. (2018) ‘Fever of unknown origin in adults: a 20-year retrospective study’, Scandinavian Journal of Infectious Diseases, 50(6), pp. 461–468. Available at: https://pubmed.ncbi.nlm.nih.gov/29451084/
- Walter, E.J., Hanna-Jumma, S., Carraretto, M. and Forni, L. (2016) ‘The physiological effects and therapeutic applications of heat stroke’, Best Practice & Research Clinical Anaesthesiology, 30(4), pp. 559–569. Available at: https://pubmed.ncbi.nlm.nih.gov/27808532/
- Zenone, T. (2012) ‘Fever of unknown origin in adults: forty years after classic studies’, Current Clinical Pharmacology, 7(3), pp. 224–230. Available at: https://pubmed.ncbi.nlm.nih.gov/22524197/