

What is Basal Cell Carcinoma? Introduction and Epidemiology
Basal Cell Carcinoma (BCC) (other names – basalioma, rodent ulcer) represents approximately 80% of all non-melanoma skin cancers (NMSC). While historically associated with geriatric populations, incidence rates are rising globally, particularly in women under 40, likely attributed to changes in sun exposure habits and the prevalence of indoor tanning.
Unlike Melanoma, which poses a high risk of systemic metastasis, BCC is primarily a disease of local destruction.
The tumor grows via direct extension, eroding skin, cartilage, muscle, and eventually bone.
For this reason, it was historically termed a “Rodent Ulcer,” as it appeared to gnaw away the flesh.
The “H-Zone” Danger
While BCC can occur anywhere, 80% of lesions are found on the head and neck. The highest risk area is the mid-facial “H-Zone” (nasolabial folds, nose, eyelids, ear canal).
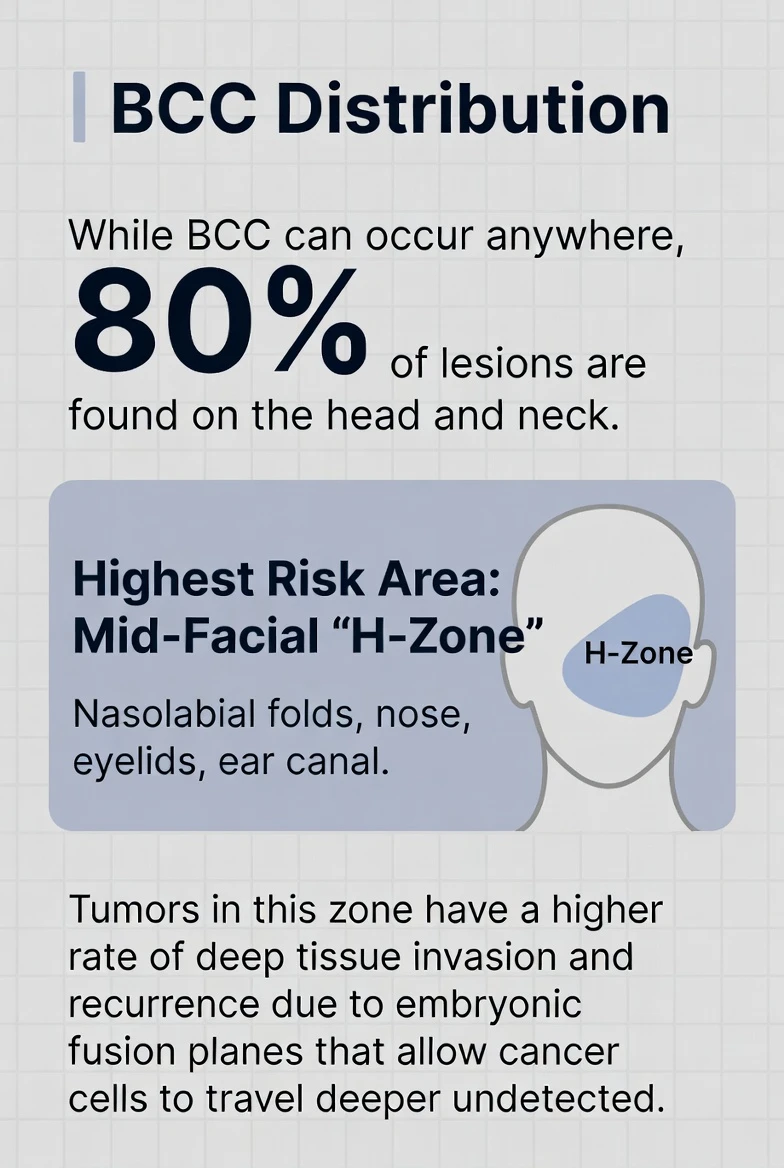
Tumors in this zone have a higher rate of deep tissue invasion and recurrence due to embryonic fusion planes that allow cancer cells to travel deeper undetected.
Basalioma Etiology and Pathogenesis
Knowing why BCC forms is critical for prevention and targeted therapy.
The Role of Ultraviolet (UV) Radiation
The primary carcinogen is UV radiation, specifically intermittent, intense exposure (the kind that causes sunburns), especially during childhood and adolescence.
- UVB (290–320 nm): Directly damages DNA, causing specific mutations (C-to-T transitions).
- UVA (320–400 nm): Penetrates deeper, causing oxidative stress and suppressing the skin’s local immune system, allowing tumor cells to escape detection.
Latency Period: There is often a 20–50 year lag between the UV damage and the clinical appearance of the tumor. This explains why patients in their 80s present with BCCs caused by sun exposure from their 20s.
Molecular Genetics
The hallmark of Basal Cell Carcinoma is the dysregulation of the Hedgehog Signaling Pathway.
- Normal Function: In healthy skin, a gene called PTCH1 acts as a suppressor (a brake), preventing the cell from dividing unless necessary.
- The Mutation: UV damage causes a “loss of function” mutation in PTCH1.
- The Result: Without the PTCH1 brake, the protein Smoothened (SMO) becomes constitutively active. This sends a constant “GO” signal to the nucleus, causing basal cells to proliferate uncontrollably.
Clinical Relevance: Discover of this pathway led to the development of Hedgehog Pathway Inhibitors (like Vismodegib), oral chemotherapy drugs used for inoperable BCCs that essentially turn the “brake” back on.
Clinical Subtypes of Basalioma: A Visual Atlas
BCC is a chameleon. It has five distinct clinical presentations. Misdiagnosing the subtype leads to treatment failure, as aggressive subtypes require wider surgical margins.
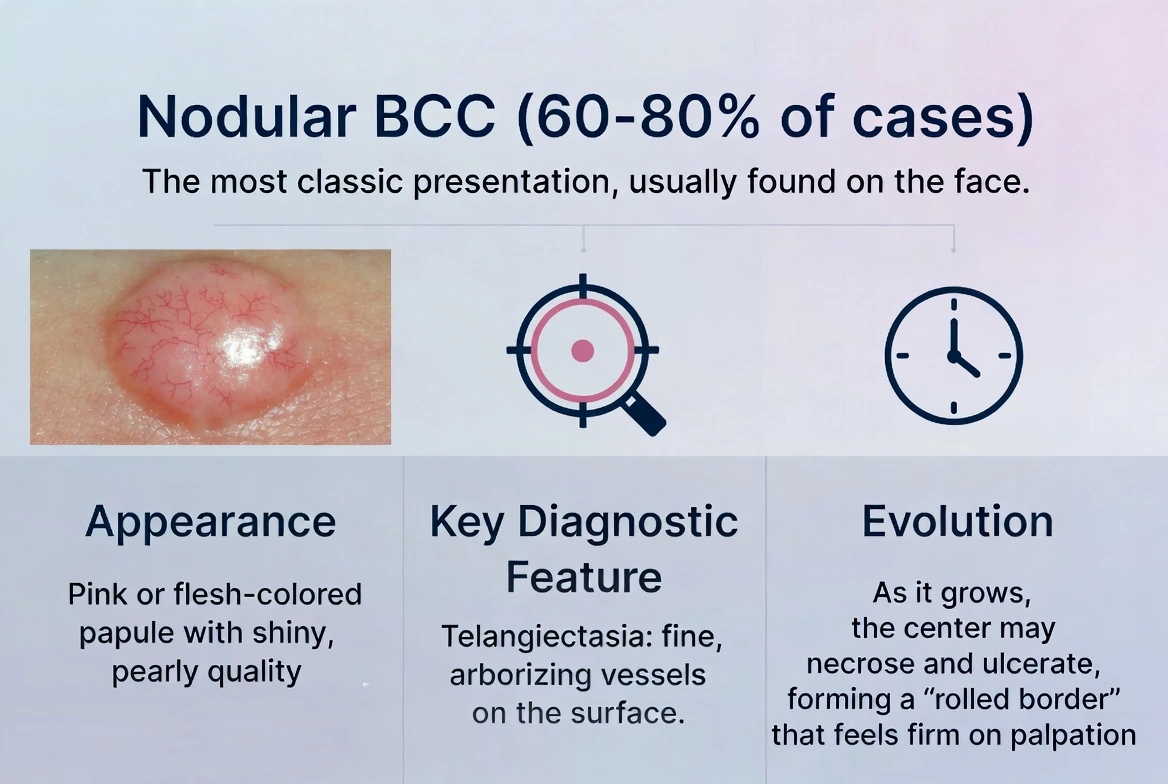
A. Nodular BCC (60–80% of cases)
The most classic presentation, usually found on the face.
- Appearance: A pink or flesh-colored papule (bump) with a shiny, pearly quality.
- Key Diagnostic Feature: Telangiectasia. Fine, arborizing blood vessels can be seen stretching over the surface of the tumor.
- Evolution: As it grows, the center often undergoes necrosis and ulcerates, leaving a “rolled border” that feels firm to the touch.
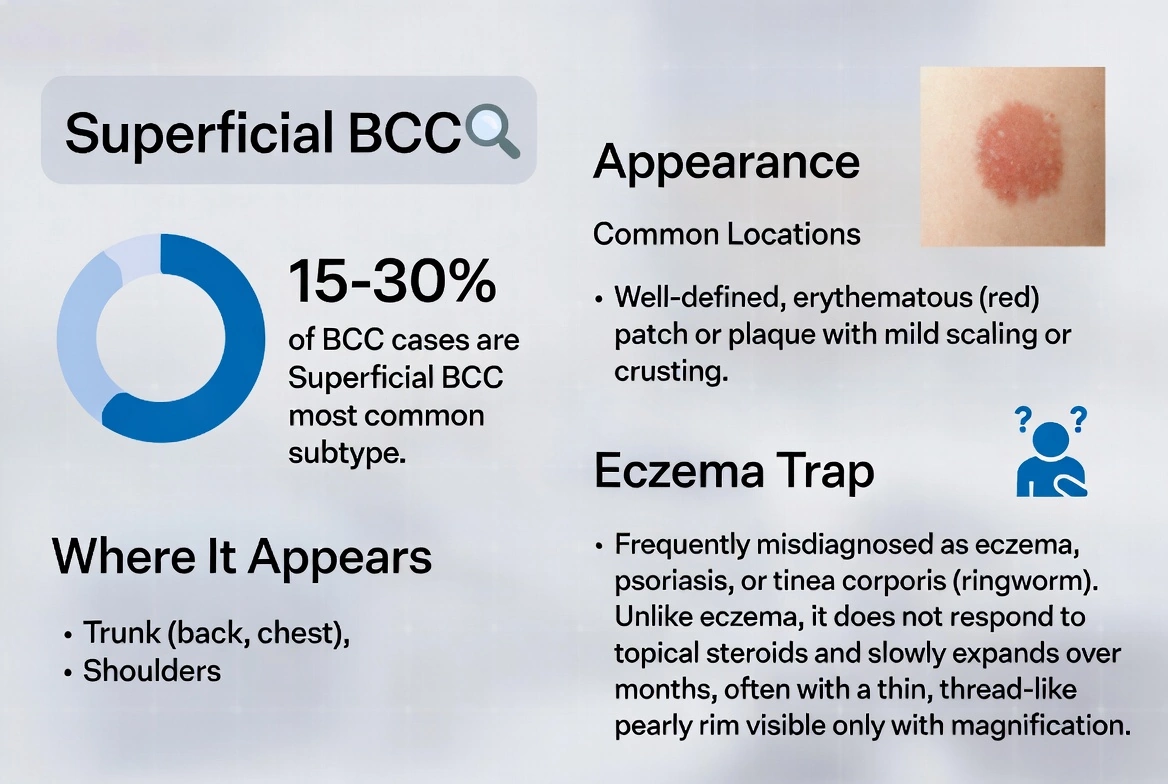
B. Superficial BCC (15–30% of cases)
Most common on the trunk (back, chest) and shoulders.
- Appearance: A well-defined, erythematous (red) patch or plaque. It often has mild scaling or crusting.
- The “Eczema Trap”: It is frequently misdiagnosed as eczema, psoriasis, or tinea corporis (ringworm).
- Differentiation: Unlike eczema, Superficial BCC will not respond to topical steroids and will slowly expand over months. It often has a thin, thread-like pearly rim visible only with magnification.
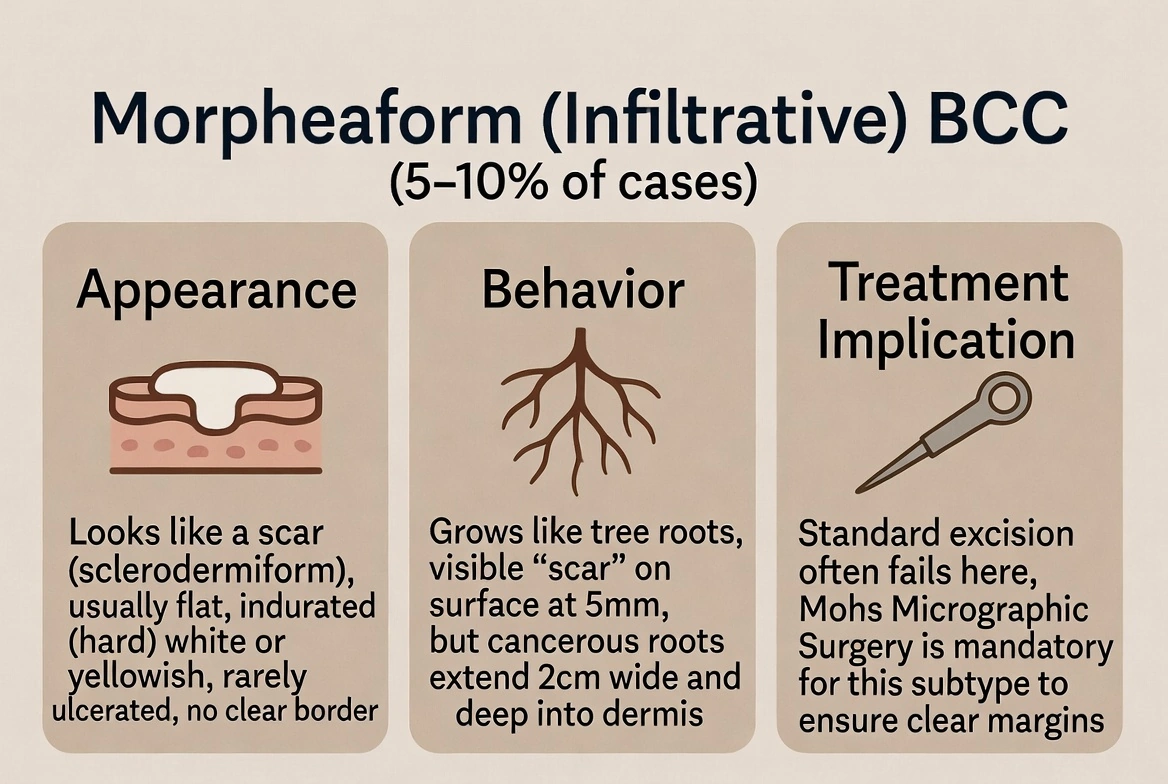
C. Morpheaform (Infiltrative) BCC (5–10% of cases)
This is the most dangerous and deceptive subtype.
- Appearance: It looks like a scar (sclerodermiform). It is usually a flat, indurated (hard), white or yellowish plaque. It is rarely ulcerated and has no clear border.
- Behavior: The tumor grows like tree roots. The visible “scar” on the surface may be 5mm, but the cancerous roots may extend 2cm wide and deep into the dermis.
- Treatment Implication: Standard excision often fails here. Mohs Micrographic Surgery is mandatory for this subtype to ensure clear margins.
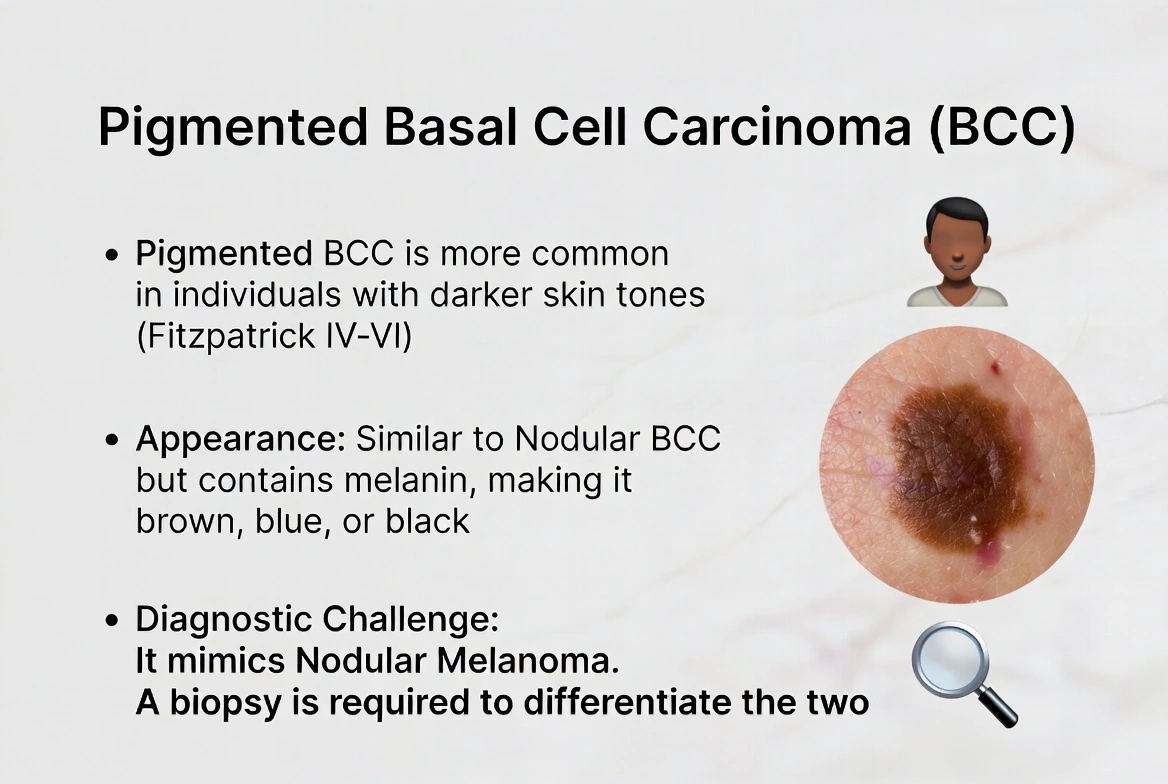
D. Pigmented BCC
Seen more frequently in people with deeper skin pigmentation, typically classified as Fitzpatrick types IV to VI.
- Appearance: Similar to Nodular basalioma but contains melanin, making it brown, blue, or black.
- Diagnostic Challenge: It mimics Nodular Melanoma. A biopsy is required to differentiate the two.
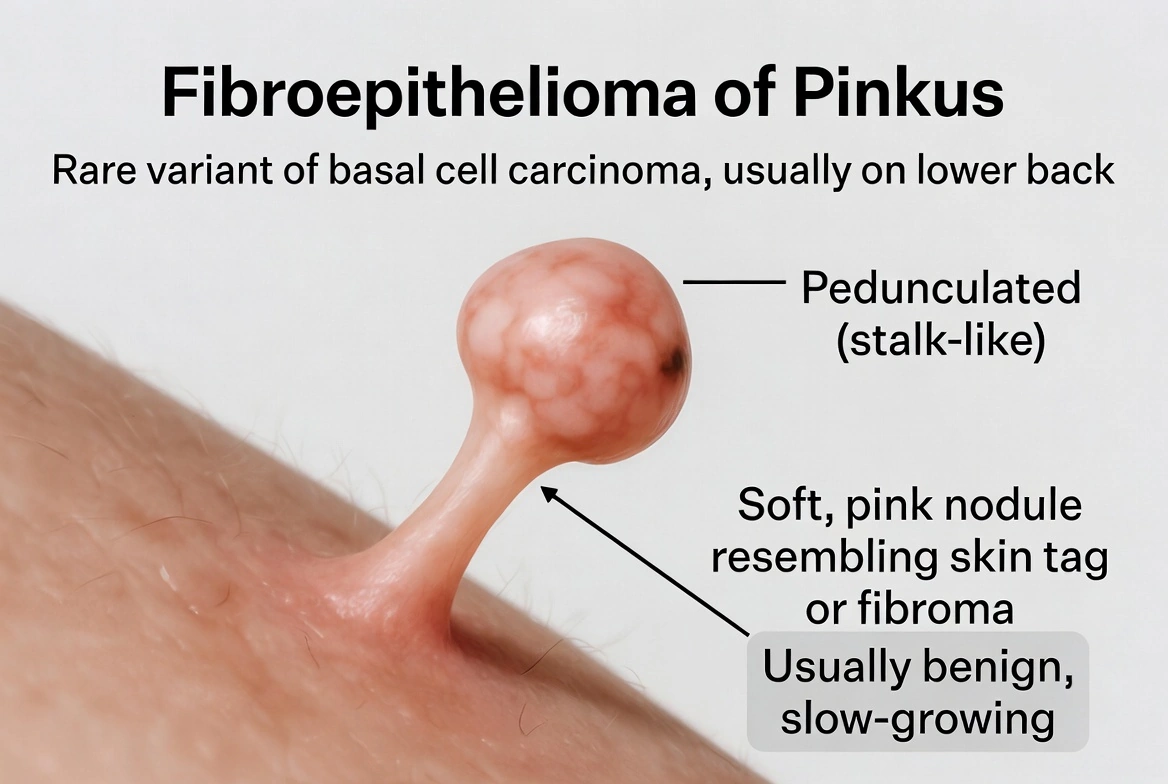
E. Basalioma type – Fibroepithelioma of Pinkus
A rare variant, usually found on the lower back.
- Appearance: A pedunculated (stalk-like), soft, pink nodule that resembles a skin tag or fibroma.
Diagnostic of Basal Cell Carcinoma
1. Dermoscopy: The Specialist’s View
 Dr. S. Prikhodko:
Dr. S. Prikhodko:
Dermoscopy (epiluminescence microscopy) allows the dermatologist to view structures below the stratum corneum. For BCC, specific patterns confirm the diagnosis with 95% accuracy.
- Arborizing Vessels: Bright red vessels that branch like trees, coming into sharp focus. (Indicative of Nodular BCC).
- Blue-Gray Ovoid Nests: Large clumps of pigmented tumor cells floating in the dermis.
- Maple Leaf-Like Areas: Brown or gray extensions at the periphery of the lesion, resembling leaves. (Common in Superficial BCC).
- Spoke-Wheel Areas: Radial projections usually connected to a central dark hub.
- Absence of Pigment Network: BCC lacks the reticular pigment network typically seen in melanocytic lesions (moles and melanoma).
2. Histopathology
When the tissue is sent to the lab, the pathologist looks for specific architectural patterns.
- Basaloid Cells: The tumor is composed of islands of cells with large, dark blue nuclei (hyperchromatic) and very little cytoplasm.
- Peripheral Palisading: The cells at the outer edge of the tumor nest line up in parallel, resembling a picket fence.
- Retraction Artifact: A white “cleft” or gap separates the tumor island from the surrounding stroma (connective tissue). This is a classic hallmark of BCC caused by tissue shrinkage during processing.
- Mucinous Stroma: The tissue surrounding the tumor is often rich in mucin, which explains why the tumor often falls apart or feels “mushy” during curettage.
Differential Diagnosis of Basalioma
Before treatment, the clinician must rule out conditions that mimic BCC.
| Condition | Distinguishing Feature from BCC |
|---|---|
| Sebaceous Hyperplasia | Enlarged oil glands. They are yellowish (not pearly) and often have a central dell. Common in oily skin zones. |
| Squamous Cell Carcinoma | Grows faster. Usually tender/painful. Has a thick, rough keratin scale (hyperkeratosis) rather than a smooth surface. |
| Amelanotic Melanoma | A pink bump with no pigment. This is the most critical differential. Dermoscopy shows “milky-red areas” and polymorphous vessels, not arborizing vessels. |
| Lichen Planoid Keratosis | A benign lesion that can look like a superficial BCC but usually regresses on its own. |
Basal Cell Carcinoma Treatment Protocols
Treatment choice depends on the Risk Stratification of the tumor. We categorize tumors based on location, size, and subtype.
A. Surgical Modalities
1. Mohs Micrographic Surgery
- Indication: High-risk tumors on the face (H-Zone), recurrent tumors, or Morpheaform subtype.
- Technique: The surgeon removes the visible tumor and immediately maps and freezes the tissue to examine 100% of the margins under a microscope. If cancer cells remain, another thin layer is taken only from that specific area.
- Advantage: Highest cure rate (99%) and maximum tissue preservation.
2. Standard Surgical Excision
- Indication: Low-risk tumors on the trunk or extremities (arms/legs).
- Technique: The tumor is removed with a safety margin of clinically healthy skin (usually 4mm).
- Cure Rate: ~95% for primary lesions.
B. Destructive Therapies (Non-Excisional)
1. Electrodessication and Curettage (ED&C)
- Indication: Small, superficial, or nodular BCCs on low-risk areas (back/shoulders).
- Technique: The tumor is scraped away (curetted) and the base is burned (dessicated).
Note: This technique relies on the “mushy” texture of basalioma to define the border. It is contraindicated for Morpheaform BCC or facial lesions, as it leaves a round white scar and has no margin control.
2. Cryosurgery (Liquid Nitrogen)
- Indication: Superficial basaliomas, or patients who are poor surgical candidates (e.g., elderly patients on blood thinners).
- Technique: Liquid nitrogen (-196°C) is applied to freeze the tumor cells, causing necrosis.
Author’s Note (Dr. Prikhodko): “Cryosurgery is an underutilized tool in geriatric oncology. While it lacks the histological confirmation of excision, the Prikhodko Method demonstrates that a double freeze-thaw cycle can achieve cure rates comparable to excision for selected low-risk tumors, with significantly less morbidity for frail patients.”C. Topical & Photodynamic Therapies
Used strictly for Superficial BCCs.
- Imiquimod (Aldara): An immune-response modifier cream that stimulates the patient’s own immune system to attack the cancer.
- 5-Fluorouracil (Efudex): A topical chemotherapy that interferes with DNA synthesis in rapidly dividing cells.
- Photodynamic Therapy (PDT): A photosensitizing agent (ALA) is applied, followed by exposure to blue or red light, destroying the tumor cells.
Prognosis and Follow-Up
Metastasis
Metastatic BCC is exceedingly rare (0.0028% to 0.55%). When it occurs, it usually spreads to the regional lymph nodes, lungs, or bones. The risk is higher in tumors >2cm that have been neglected for years.
Recurrence
The primary risk of BCC is local recurrence.
- 5-Year Recurrence Rate (Primary): ~1.0% with Mohs surgery, ~10% with standard excision.
- 5-Year Recurrence Rate (Recurrent): If a tumor has already been treated and comes back, the risk of it returning again jumps to 17-30%.
Patient Surveillance
Patients with a history of basalioma have a 40% risk of developing a new primary BCC within 5 years.
Protocol: Full body skin exam every 6 months for 2 years, then annually.
Caregiver & Nursing Perspectives In Dealing With Basalioma
1. The “Pimple That Won’t Heal”
The most common history I hear from patients is: “I thought it was a shaving cut” or “I thought it was a pimple.”
2. Managing “Watch and Wait” in the Elderly
In patients over 80 with significant comorbidities, the decision to operate is not automatic. A slow-growing Nodular BCC might take 5 years to grow 1cm.
If the patient has advanced dementia or end-stage heart failure, palliative care (keeping the lesion clean and covered) may be superior to the trauma of surgery.
This decision requires a candid conversation between the Oncologist and the family.
3. Post-Procedure Wound Care
Whether treated by Mohs or Curettage, BCC removal leaves an open wound or an incision.
- Moist Healing: Contrary to old beliefs (“let it air out”), wounds heal 50% faster and with less scarring if kept moist (covered with Petrolatum/Vaseline) and covered.
- Sun Protection: A fresh scar is highly susceptible to UV damage. Hyperpigmentation (permanent darkening) can occur if the healing wound is exposed to the sun.
References
- National Comprehensive Cancer Network (NCCN). Clinical Practice Guidelines in Oncology: Basal Cell Skin Cancer. Version 2.2024. Available at: nccn.org
- Bolognia, J. L., et al. Dermatology. 4th Edition. Elsevier, 2018. (Chapter 108: Basal Cell Carcinoma).
- Prikhodko S.G. Clinical and Surgical Treatment of Basal Cell Carcinoma of the Head and Neck in Outpatient Settings. (PhD Thesis). Pavlov First Saint Petersburg State Medical University, 1988.
- Marzuka, A. G., & Book, S. E. Basal cell carcinoma: pathogenesis, epidemiology, clinical features, diagnosis, histopathology, and management. Yale J Biol Med. 2015;88(2):167-179.
- American Academy of Dermatology. Guidelines of care for the management of basal cell carcinoma. J Am Acad Dermatol. 2018;78(3):540-559.
- Rubin, A.I., et al. Basal-Cell Carcinoma. N Engl J Med 2005; 353:2262-2269.