

1. Executive Overview
Squamous Cell Carcinoma (SCC) is the second most prevalent form of skin cancer worldwide, distinguished by its origin in the squamous cells—the flat, scale-like keratinocytes that comprise the outermost layers of the epidermis. Unlike its more common counterpart, Basal Cell Carcinoma, SCC exhibits more aggressive biological behavior with a genuine capacity for metastatic spread to regional lymph nodes and distant organs, occurring in approximately 2-5% of cases. This malignancy develops forming the skin’s outer layer—begin growing abnormally and uncontrollably.
 Dr. Sergey Prikhodko: In my practice, I distinguish between ‘Sun-Induced SCC’ and ‘Scar-Induced SCC’ (Marjolin’s Ulcer). While sun-induced tumors are common on the face, SCC can also arise in old burn scars or chronic leg ulcers. These ‘Scar SCCs’ are biologically more aggressive and have a higher rate of metastasis than those caused by the sun.
Dr. Sergey Prikhodko: In my practice, I distinguish between ‘Sun-Induced SCC’ and ‘Scar-Induced SCC’ (Marjolin’s Ulcer). While sun-induced tumors are common on the face, SCC can also arise in old burn scars or chronic leg ulcers. These ‘Scar SCCs’ are biologically more aggressive and have a higher rate of metastasis than those caused by the sun.Signs & Symptoms of SCC
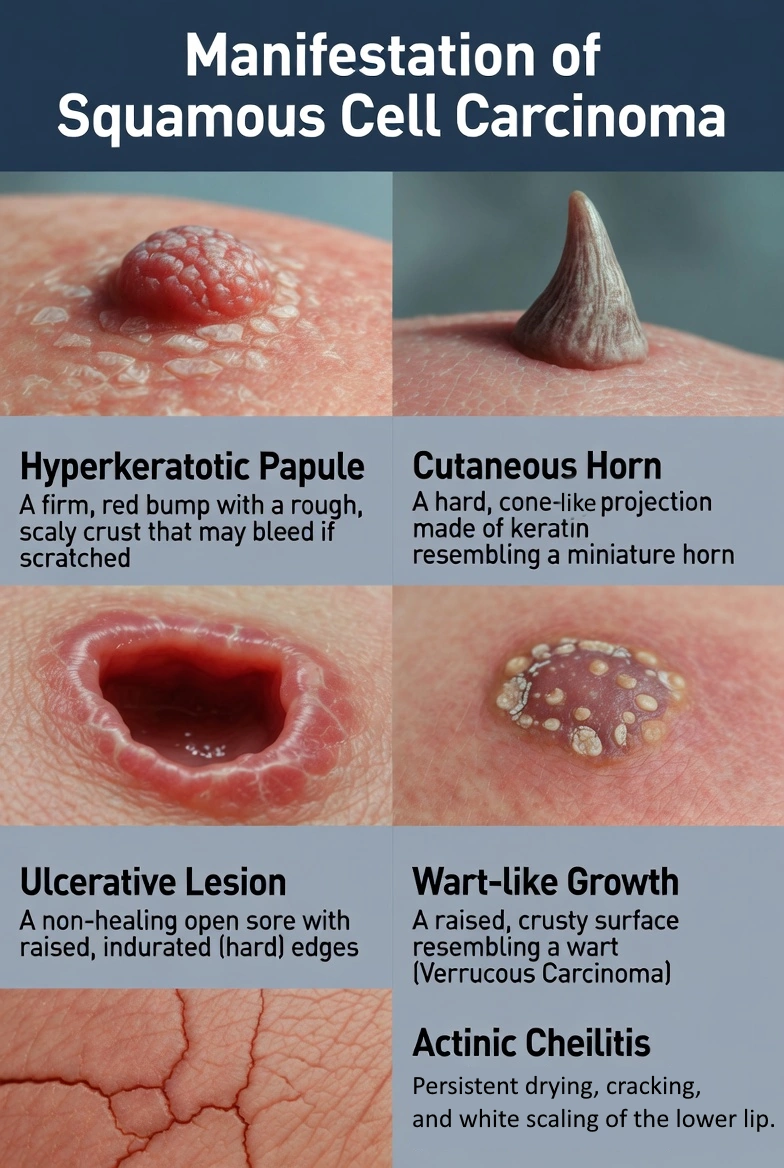
Recognizing Squamous Cell Carcinoma early is the key to preventing metastasis. Unlike the “pearly” appearance of Basal Cell Carcinoma, SCC is typically keratotic (crusty/scaly).
| Symptom | Clinical Description | Dr. Prikhodko’s Diagnostic Note |
|---|---|---|
| Hyperkeratotic Papule | A firm, red bump with a rough, scaly crust. It may bleed if scratched. | “f the scab is removed and reappears thicker within a week, it may be a sign of squamous cell carcinoma (SCC).” |
| Cutaneous Horn | A hard, cone-shaped projection made of keratin (looks like a miniature horn). | “Always biopsy the base of a horn. 15% of them hide an invasive SCC at the bottom.” |
| Ulcerative Lesion | A non-healing open sore with raised, indurated (hard) edges. | “People often take it for a diabetic sore, but the difference is that this type of wound lacks the surrounding vascular changes.” |
| Wart-like Growth | A raised, crusty surface resembling a wart (Verrucous Carcinoma). | “Unlike a common viral wart, this kind of lesion tends to feel hard to the touch and may cause tenderness or mild discomfort.” |
| Actinic Cheilitis | Persistent drying, cracking, and white scaling of the lower lip. | “This is SCC in-situ of the lip. It requires immediate treatment to prevent invasion into the lip muscle.” |
The “Ugly Duckling” & Tenderness Rule
While the “Ugly Duckling” rule (a spot that looks different from the rest) is often cited for Melanoma, it applies here too. However, the most specific sign for SCC is Tenderness.
Etiology: Root Causes & Risk Factors
Primary Environmental Factors
- Cumulative Sun Exposure: Unlike Melanoma, which is linked to intense sunburns, SCC is linked to cumulative exposure over a lifetime. This includes outdoor workers, golfers, and those living in sunny climates.
- Tanning Beds: Artificial UV radiation significantly increases risk, particularly when use begins before age 30.
- Radiation Exposure: Previous radiation therapy for other cancers can induce SCC in the treatment field years later.
- Chemical Exposure: Historical contact with arsenic (found in old well water or pesticides) or coal tar.
Host Factors (Genetics & Health)
- Fair Skin phenotype: Less melanin offers less protection against DNA damage.
- Immunosuppression: This is the strongest risk factor. Organ transplant recipients taking anti-rejection meds (like Cyclosporine) have a 65 to 250 times higher risk of developing aggressive SCCs.
- Genetic Syndromes: Conditions like Xeroderma Pigmentosum (inability to repair DNA) or Albinism.
- HPV Infection: Certain strains of Human Papillomavirus are linked to SCCs in the genital and oral regions.
Diagnosis of Squamous Cell Carcinoma
1. Visual Examination & Dermoscopy
Using a dermatoscope, the specialist looks for specific vascular patterns.
2. The Biopsy
To confirm diagnosis, tissue must be examined.
- Shave Biopsy: For superficial lesions.
- Punch Biopsy: For deeper lesions (to assess depth of invasion).
- Excisional Biopsy: Removing the whole lesion for diagnosis and treatment simultaneously.
3. Histopathology (Under the Microscope)
Dr. S. Prikhodko:
This is what the pathologist sees that confirms the diagnosis:
- Keratin Pearls: Concentric layers of keratinization (onion-skin appearance) deep in the dermis. This is the hallmark of well-differentiated SCC.
- Atypia: Nuclear pleomorphism (cells of different sizes) and hyperchromasia (dark nuclei).
- Dermal Invasion: Strands of atypical keratinocytes breaking through the basement membrane.
What can you do for a self-check?
Monthly skin self-checks save lives:
- Use good lighting and a full-length mirror
- Examine all areas: Don’t forget scalp, behind ears, between toes, genital area
- Use a hand mirror for hard-to-see spots
- Take photos of concerning areas to track changes
- Know your skin: Familiarity helps you spot new or changing lesions
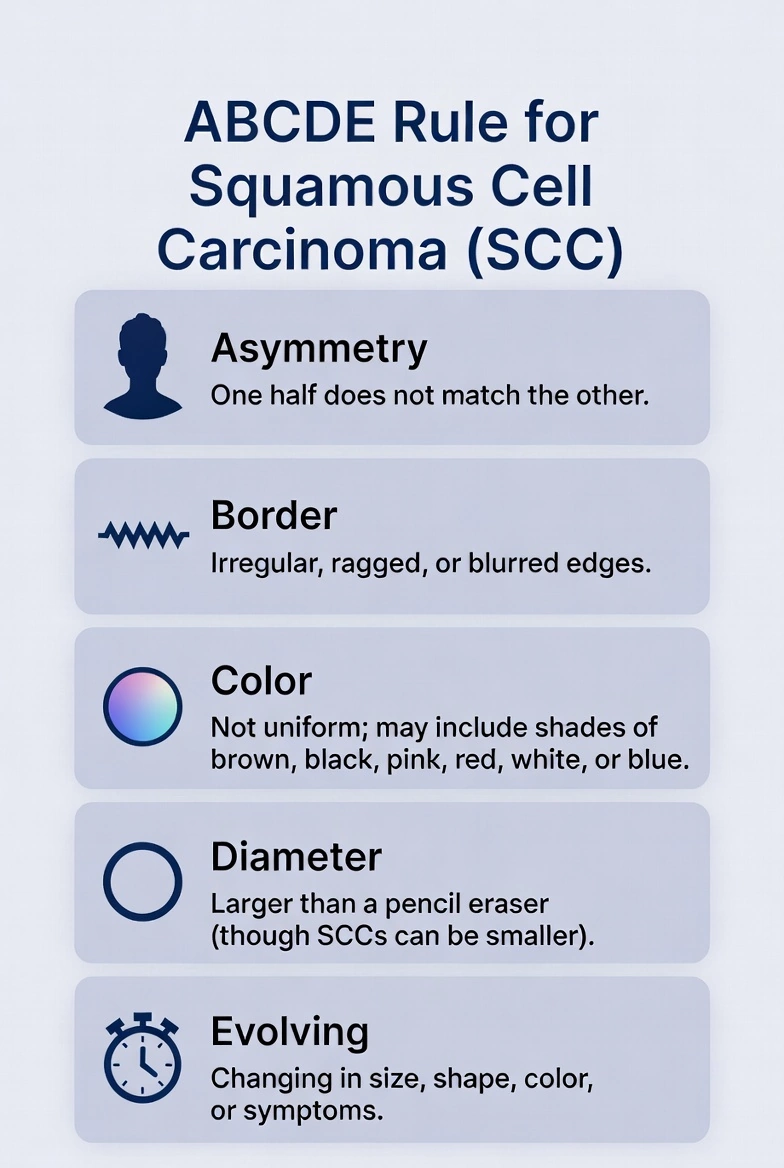
The ABCDE rule (helpful for melanoma, but also useful for general skin awareness):
- Asymmetry: One half doesn’t match the other
- Border: Edges are irregular, ragged, or blurred
- Color: Color isn’t uniform; may include shades of brown, black, pink, red, white, or blue
- Diameter: Larger than a pencil eraser (though SCCs can be smaller)
- Evolving: Changing in size, shape, color, or symptoms
SCC Treatment: Clinical Protocols
Treatment of Squamous Cell Carcinoma is selected based on the size, location, and histological subtype of the tumor.
Surgical Modalities (Standard of Care)
| Treatment | Mechanism | Indication | Dr. Prikhodko’s Note |
|---|---|---|---|
| Standard Excision | Cutting out the tumor with a 4-6mm margin. | Low-risk tumors on trunk/arms. | “Simple, effective, and allows for margin checking.” |
| Mohs Surgery | Layer-by-layer removal with 100% margin control. | Face, Ears, Lips, or Recurrent tumors. | “Mandatory for facial tumors to preserve anatomy.” |
| Curettage & Desiccation | Removing the tumor by scraping it away and then cauterizing the remaining base. | Small, superficial SCCs. | “Only for in situ disease. Risky for invasive tumors.” |
Non-Surgical & Advanced Options
1. Cryotherapy (Liquid Nitrogen)
Freezing the cancer cells.
2. Radiation Therapy
High-energy rays kill cancer cells. Used for elderly patients who cannot tolerate surgery, or as adjuvant therapy for tumors that have wrapped around nerves (perineural invasion). This type of therapy is useful in case of metastatic spread.
3. Immunotherapy
For metastatic cases, drugs like Cemiplimab (PD-1 inhibitors) help the body’s immune system attack the cancer.
Nursing & Home Care Guide
1. Post-Op Wound Management
The Crust: SCC surgeries often weep a yellow fluid. This creates a crust. Do not pick it; this is fibrin, a biological bandage.
Moist Healing: The most common mistake patients make is letting the wound “air out.” A dry wound scabs, scars, and heals 50% slower. Keep it covered with a thin layer of Petrolatum (Vaseline) and a clean bandage.
2. Monitoring for Metastasis
Because SCC can spread, your role as a patient/caregiver includes monitoring lymph nodes.
The Monthly Check: Once a month, gently feel the lymph nodes in the neck (if the cancer was on the head) or armpits (if on the arm). If you feel a hard, rubbery lump, contact your oncologist immediately.
3. Sun Protection for Survivors
A person who has had one SCC has a 50% chance of getting another.
Comparison: Squamous Cell Carcinoma vs. Basal Cell Carcinoma
| Feature | Squamous Cell Carcinoma (SCC) | Basal Cell Carcinoma (BCC) |
|---|---|---|
| Frequency | Second most common skin cancer | Most common skin cancer |
| Cell origin | Squamous cells (outer skin layers) | Basal cells (deeper in outer skin layer) |
| Typical appearance | Scaly red patches, open sores, wart-like growths; often rough texture | Pearly bumps, pink growths, open sores that don’t heal; often shiny or waxy |
| Common locations | Sun-exposed areas: face, ears, neck, hands | Sun-exposed areas, especially face and neck |
| Growth speed | Can grow relatively quickly | Usually slow-growing |
| Metastasis risk | Can spread to lymph nodes/organs (2-5% of cases) | Rarely spreads (extremely uncommon) |
| Local invasion | Can grow deep into tissues | Can grow deep and cause local damage but rarely spreads |
| Recurrence after treatment | Moderate risk | Low to moderate risk |
| Treatment approaches | Similar to BCC: surgery most common; Mohs surgery for high-risk | Surgery most common; various options depending on size/location |
| Cure rate when caught early | >90% | >95% |
Frequently Asked Questions about Squamous Cell Carcinoma (FAQs)
How preventable is squamous cell carcinoma?
A: Highly preventable. Since cumulative UV exposure is the driver, studies show that consistent daily sunscreen use can reduce SCC risk by 40%. It is never “too late” to start; protecting the skin now prevents further DNA damage.
Is it normal to get more than one skin cancer?
A: Yes. This is called “Field Cancerization.” The sun damage covers the whole area (like the whole face), so multiple cancers may pop up in the same “field” over time. 30-50% of patients develop a second cancer within 5 years.
How quickly does SCC grow?
A: Growth rates vary. Some develop over months, others over years. What matters most: don’t wait to see if something grows. Have any suspicious spot checked promptly
What is the difference between Actinic Keratosis and SCC?
A: Think of them as a continuum. Actinic Keratosis (AK) is a precancerous lesion (Stage 0). If left untreated, about 10% of AKs transform into invasive Squamous Cell Carcinoma. Treating AKs with liquid nitrogen is essentially cancer prevention.
Should I worry about SCC spreading?
A: For most small skin lesions, the risk is low. However, you should worry if the tumor is >2cm, located on the ear or lip, or if you are immunosuppressed. In these high-risk cases, the metastasis rate can rise to 10-20%.
Can dark-skinned people get squamous cell carcinoma?
A: Yes. While less common in people with darker skin tones due to melanin’s protective effects, SCC absolutely occurs in all skin types. In darker-skinned individuals, SCCs more commonly develop in non-sun-exposed areas, chronic wounds, or scars, and may be diagnosed at later stages. Everyone should practice skin awareness.
How soon after noticing something should I see a doctor?
A: Don’t wait. Schedule an appointment within a few weeks of noticing a persistent skin change. While not every spot is cancer, early professional evaluation provides peace of mind or, if cancer is present, the best chance for simple, effective treatment.
Does health insurance cover removal?
A: Yes. Unlike cosmetic mole removal, the treatment of SCC is a medical necessity and is covered by standard insurance plans and Medicare.
Full References & Sources
- National Comprehensive Cancer Network (NCCN). Squamous Cell Skin Cancer Guidelines. Version 1.2025. – https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1466
- Prikhodko S.G. Metatypical Skin Cancer and Aggressive Growth Patterns. Bulletin of Dermatology. 1986.
- MedlinePlus. Squamous Cell Carcinoma. National Library of Medicine. Available at: medlineplus.gov/skincancer.html – https://medlineplus.gov/ency/article/000829.htm
- Waldman A., Schmults C. Cutaneous Squamous Cell Carcinoma of the High-Risk Patient. J Am Acad Dermatol. 2019. – https://pubmed.ncbi.nlm.nih.gov/30315878/
- American Academy of Dermatology. Squamous Cell Carcinoma Treatment. – https://www.aad.org/public/diseases/skin-cancer/types/common/scc/treatment
- Mayo Clinic. Squamous cell carcinoma of the skin. – https://www.mayoclinic.org/diseases-conditions/squamous-cell-carcinoma/symptoms-causes/syc-20352480
For questions about this content or to report errors, contact your healthcare provider or visit the referenced medical sources directly.