What Is Osteosarcoma?
Osteosarcoma is a type of bone cancer that starts in the cells that form new bone. It most often appears in the long bones of the arms or legs, especially around the knee or shoulder. Although it can occur at any age, the disease is most frequently diagnosed in teenagers and young adults during periods of rapid bone growth.
The tumor destroys healthy bone tissue and can spread (metastasize) to other parts of the body, most commonly the lungs. Early detection and prompt treatment improve the chances of a good outcome.
Who Is at Risk?
While the exact cause of osteosarcoma is unknown, several factors have been linked to a higher chance of developing the disease.
| Risk Factor | Details |
|---|---|
| Age | Most cases appear between 10 and 30 years old, with a peak during the teenage growth spurt. |
| Sex | Slightly more common in males than females. |
| Height | Taller individuals have a modestly increased risk, possibly related to faster bone growth. |
| Prior Radiation Therapy | Exposure to high-dose radiation for another cancer can raise risk years later. |
| Genetic Conditions | Disorders such as Li-Fraumeni syndrome, hereditary retinoblastoma (RB1 gene mutation), and Bloom syndrome are associated with higher odds. |
| Bone Diseases | Conditions like Paget’s disease of bone (in older adults) may precede osteosarcoma. |
| Family History | Having a close relative with osteosarcoma or another sarcoma slightly increases risk. |
Note: Most people with these risk factors never develop osteosarcoma, and many patients have no identifiable risk factor at all.
Common Signs and Symptoms of Osteoscarcoma
Symptoms often develop slowly and may be mistaken for ordinary growing pains or a sports injury. Persistent warning signs include:
- Localized pain that worsens at night or with activity
- Swelling or a lump near the affected bone, sometimes warm to the touch
- Limping or difficulty moving the joint nearby
- Unexplained bone fracture after minor trauma (pathologic fracture)
- Fatigue or unintentional weight loss (less common, may appear later)
Important!If any of these symptoms last more than a few weeks or worsen, it is important to seek medical evaluation promptly.
How Doctors Make the Diagnosis
A stepwise approach helps confirm osteosarcoma and rule out other conditions.
- Medical history and physical exam – The clinician asks about symptom onset, activity level, family history, and performs a careful exam of the painful area.
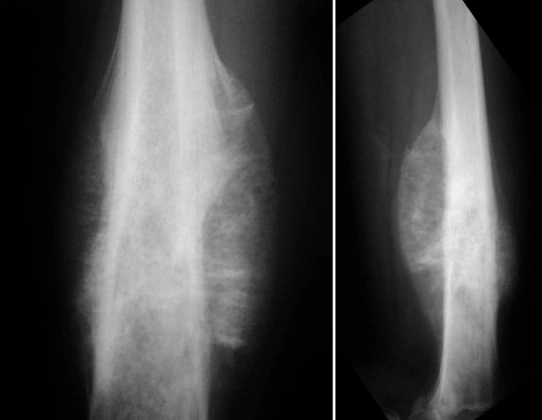
- Imaging studies
- X-ray – Often the first test; may show a destructive lesion with a “sun-burst” pattern or new bone formation.
- Magnetic Resonance Imaging (MRI) – Provides detailed view of the tumor’s extent within the bone and surrounding soft tissues.
- Computed Tomography (CT) scan – Useful for checking the lungs for metastatic spots.
- Bone scan – Highlights areas of increased bone activity throughout the skeleton.
- Biopsy – A small sample of tissue is taken (either with a needle or through a small incision) and examined under a microscope. The biopsy confirms the presence of malignant bone-forming cells and helps differentiate osteosarcoma from other bone tumors.
- Laboratory tests – Blood work (such as lactate dehydrogenase, alkaline phosphatase) may be ordered to assess overall health and monitor treatment response, though no blood test alone can diagnose osteosarcoma.
The pathology report will note the tumor’s grade (how abnormal the cells look) and histologic subtype (e.g., conventional, telangiectatic, small-cell, low-grade central).
Staging the Osteosarcoma
Staging describes how far the cancer has spread and guides treatment choices. Two systems are commonly used:
- the TNM system (tumor, nodes, metastasis)
- Enneking system (used mainly for musculoskeletal tumors).
Enneking Staging (most relevant for osteosarcoma)
| Stage | Definition | Typical Features |
|---|---|---|
| IA | Low-grade tumor, confined to the bone (intracompartmental) | Small, well-defined lesion; low mitotic activity |
| IB | Low-grade tumor, extends beyond the bone cortex (extracompartmental) | Same low-grade features but with soft-tissue involvement |
| IIA | High-grade tumor, confined to the bone | Aggressive appearance, still inside bone |
| IIB | High-grade tumor, with extraosseous extension | High-grade cells break through bone cortex |
| III | Any grade with distant metastasis (most often lungs) | Presence of lung nodules or other organ spread |
TNM Staging (simplified)
| Component | Meaning |
|---|---|
| T (Tumor size) | T1: ≤8 cm; T2: >8 cm; T3: multiple separate tumor sites in the same bone |
| N (Nodes) | N0: no regional lymph node involvement; N1: lymph nodes positive |
| M (Metastasis) | M0: no distant spread; M1: distant metastasis present (commonly lungs) |
Combining T, N, and M yields stages I–IV, with higher numbers indicating more extensive disease.
Treatment Options
Treatment usually combines chemotherapy, surgery, and sometimes radiation therapy. The exact plan depends on tumor stage, location, size, and the patient’s overall health.
Neoadjuvant Chemotherapy
- Goal: Shrink the tumor before surgery, treat microscopic spread, and assess tumor response.
- Common regimens:
- MAP: Methotrexate, Doxorubicin (Adriamycin), Cisplatin
- Alternative: Ifosfamide and Etoposide may be added or substituted in certain protocols.
- Duration: Usually given in cycles over about 10–12 weeks before surgery.
Surgery For Osteosarcoma
| Surgical Approach | When Used | What It Involves |
|---|---|---|
| Limb-salvage surgery | Tumor amenable to removal while preserving function | The diseased bone segment is excised and replaced with a prosthetic implant, allograft (donor bone), or a combination. Soft-tissue reconstruction follows. |
| Amputation | Tumor involves major nerves/vessels, or limb-salvage not feasible | Removal of the entire limb or part of it; modern prosthetics allow high levels of activity. |
| Rotationplasty (mainly for distal femur tumors) | Specific cases in young patients | The ankle joint is rotated to function as a knee; a prosthesis replaces the lower leg. |
| Pulmonary metastasectomy | Isolated lung metastases after chemotherapy | Surgical removal of lung nodules to improve long-term control. |
Adjuvant Chemotherapy
- Goal: Eradicate any remaining cancer cells after surgery.
- Same drugs as neoadjuvant therapy, often continued for another 10–12 weeks.
- Response assessment: Pathologic examination of the resected tumor determines the percentage of necrosis (dead tumor cells). Greater necrosis (>90%) correlates with better prognosis.
Radiation Therapy
- Limited role because osteosarcoma is relatively resistant to radiation.
- Used when:
- Tumor cannot be completely removed surgically (positive margins).
- Patient declines surgery or is not a surgical candidate.
- Palliation of painful metastases (e.g., spinal lesions).
- Technique: External-beam radiation, often with conformal techniques to spare normal tissue.
New Upcoming Therapies
- Targeted therapies (e.g., inhibitors of IGF-1R, mTOR pathways) under clinical trial evaluation.
- Immunotherapy (checkpoint inhibitors, CAR-T cells) being studied, especially for refractory or metastatic disease.
- Samarium-153 or other radiopharmaceuticals for bone-targeted treatment in select cases.
Patients should discuss any trial options with their oncology team.
Managing Osteosarcoma Treatment Side Effects
Treatment can cause temporary or lasting effects. Proactive management helps maintain quality of life.
| Side Effect | Common Causes | Practical Tips |
|---|---|---|
| Nausea and vomiting | Chemotherapy (especially cisplatin, doxorubicin) | Anti-emetics prescribed before each dose; eat small, bland meals; stay hydrated. |
| Fatigue | Chemotherapy, radiation, anemia | Prioritize rest; short walks boost energy; treat anemia if present. |
| Hair loss | Cytotoxic drugs | Scalp cooling caps may reduce loss; wigs, scarves, or hats can help. |
| Mouth sores | Methotrexate, doxorubicin | Gentle oral hygiene; saline rinses; avoid spicy or acidic foods. |
| Neuropathy (numbness/tingling) | Cisplatin, vincristine (if used) | Report symptoms early; dose adjustments may be needed; physical therapy aids recovery. |
| Bone marrow suppression (low blood counts) | Chemotherapy | Regular blood tests; growth-factor support (e.g., filgrastim) for low neutrophils; transfusions for severe anemia or platelets. |
| Surgical pain & limited mobility | Post-operative healing | Pain control regimen; early physical therapy; use of assistive devices as needed. |
| Emotional distress | Diagnosis, treatment burden | Counseling, support groups, mindfulness practices; involve family and friends. |
Always inform the care team about new or worsening symptoms so they can adjust treatment promptly.
Osteosarcoma Outlook and Survival Rates
Survival statistics are based on large groups of people and cannot predict an individual’s outcome. They do, however, illustrate trends that help guide expectations.
| Factor | 5-Year Survival Approximation |
|---|---|
| Localized disease (no metastasis at diagnosis) | 60–80% |
| Metastatic disease (lung spread at diagnosis) | 20–30% |
| Good histologic response (>90% tumor necrosis after neoadjuvant chemo) | Higher end of the localized range |
| Poor histologic response (<90% necrosis) | Lower end of the localized range |
| Age < 20 years | Slightly better outcomes compared with older adults |
| Limb-salvage surgery vs. amputation | Similar survival when margins are clear; choice based on function preference |
Improvements in chemotherapy regimens and surgical techniques have raised survival rates over the past two decades. Ongoing research continues to refine treatment protocols.
Living With Osteosarcoma
A diagnosis affects not only the body but also emotions, relationships, and daily routines. Here is what you can do.
Rehabilitation and Physical Activity
- Physical therapy starts soon after surgery to restore strength, range of motion, and gait.
- Occupational therapy assists with daily tasks (e.g., dressing, schoolwork) and may recommend adaptive equipment.
- Gradual return to activity: Low-impact exercises (swimming, cycling) are often encouraged once healing permits.
Academic and Vocational Considerations
- School accommodations: Extra time for assignments, modified physical education, or home-based instruction during intensive treatment phases.
- College or work: Vocational rehab services can help with career planning, workplace adjustments, and disability benefits if needed.
9.5 Long-Term Follow-Up
After completing treatment, regular check-ups are essential:
- Physical exam every 3–4 months for the first 2–3 years, then every 6 months up to year 5, then annually.
- Imaging: Chest CT scans (to monitor lungs) and periodic X-rays or MRI of the treated bone site, as advised by the oncology team.
- Laboratory tests: To monitor organ function, especially if certain chemotherapy agents were used.
Any new pain, swelling, or respiratory symptoms should be reported promptly.
Frequently Asked Questions About Osteosarcoma
Is osteosarcoma contagious?
A: No. It cannot be spread from person to person.
Can diet or supplements cure osteosarcoma?
A: No specific diet has been proven to cure the disease. Good nutrition supports overall health and helps the body tolerate treatment, but it does not replace medical therapy.
Will I lose my limb?
A: Limb-salvage surgery is possible for many patients, especially when the tumor is detected early and responds well to chemotherapy. Amputation is reserved for cases where saving the limb would compromise safety or function.
How long does treatment last?
A: Typical courses involve about 10–12 weeks of chemotherapy before surgery, surgery itself, and another 10–12 weeks of chemotherapy afterward, for a total of roughly 6 months. Radiation, if used, may add a few extra weeks.
Can osteosarcoma come back after treatment?
A: Yes, recurrence is possible, most often in the lungs. Ongoing surveillance aims to catch any return early when it is most treatable.
Are there clinical trials I can join?
A: Many centers conduct studies on new drugs, immunotherapy approaches, or refined surgical techniques. Ask your oncologist about eligibility and any trials available at your treatment center or through national networks.
What should I tell my employer or school?
A: You have the right to privacy. Share only what you feel comfortable with; you can request accommodations through disability services or human resources without disclosing detailed medical specifics.
Helpful Resources
| Organization | What They Offer | Website |
|---|---|---|
| National Cancer Institute (NCI) | Up-to-date information on osteosarcoma, treatment guidelines, and clinical trial listings | https://www.cancer.gov/types/bone/osteosarcoma |
| MedlinePlus | Easy-to-read overview, videos, and links to trusted sources | https://medlineplus.gov/osteosarcoma.html |
| American Cancer Society (ACS) | Guides for patients, caregivers, and survivors; support service locator | https://www.cancer.org/cancer/osteosarcoma.html |
| Sarcoma Foundation of America (SFA) | Education, advocacy, patient-to-patient support, research funding | https://curesarcoma.org |
| Children’s Oncology Group (COG) | Pediatric-focused treatment protocols and trial access (relevant for adolescent patients) | https://www.childrensoncologygroup.org |
| National Institutes of Health (NIH) ClinicalTrials.gov | Searchable database of ongoing studies worldwide | https://clinicaltrials.gov |
| Local hospital cancer centers | Multidisciplinary sarcoma teams, rehabilitation services, social work, and counseling | (Check your nearest major medical center) |
Final Thoughts
Receiving a diagnosis of osteosarcoma can feel overwhelming, but many people move through treatment, regain function, and look forward to meaningful futures. Understanding the disease, knowing what to expect, and leaning on a skilled care team and supportive community are powerful steps toward healing. If you have any questions not covered here, do not hesitate to reach out to your healthcare provider—they are there to guide you, answer concerns, and help you make informed choices that fit your life and goals.
You are not alone. With knowledge, support, and expert care, many paths forward exist.
Sources & References
- Mirabello, L., Troisi, R.J. and Savage, S.A. (2009) ‘Osteosarcoma incidence and survival rates from 1973 to 2004: data from the Surveillance, Epidemiology, and End Results Program’, Cancer, 115(7), pp. 1531–1543.
- Howlader, N. et al. (eds) (2023) SEER Cancer Statistics Review, 1975–2020. Bethesda, MD: National Cancer Institute. Available at: https://seer.cancer.gov/csr/1975_2020/ (Accessed: 16 April 2026).
- Ottaviani, G. and Jaffe, N. (2009) ‘The epidemiology of osteosarcoma’, in Cancer Treatment and Research. Vol. 152. Berlin: Springer, pp. 3–13.
- Bielack, S.S. et al. (2002) ‘Prognostic factors in high-grade osteosarcoma of the extremities or trunk: an analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols’, Journal of Clinical Oncology, 20(3), pp. 776–790.
- King, A.D., Glaser, H.W. and Gorlick, R. (2020) ‘New approaches to the treatment of osteosarcoma’, Seminars in Oncology, 47(5–6), pp. 269–276.
- Marina, N.M. et al. (2004) ‘Comparison of MAPIE versus MAP in patients with localized osteosarcoma: a randomised, controlled, open-label, phase 3 trial’, The Lancet Oncology, 18(10), pp. 1384–1395.
- Whelan, J.S. and Davis, L.E. (2014) ‘Osteosarcoma, chondrosarcoma, and chordoma’, Journal of Clinical Oncology, 32(6), pp. 587–596.
- Suehara, Y. et al. (2015) ‘Genetic analysis of osteosarcoma: current status and future prospects’, International Journal of Clinical Oncology, 20(5), pp. 849–857.
- Van Maldegem, A.M. and Gelderblom, H. (2018) ‘Diagnosis and management of osteosarcoma’, European Journal of Cancer Care, 27(3), e12824.
- Lu, Y. et al. (2021) ‘Prognostic value of histologic response in osteosarcoma: a systematic review and meta-analysis’, Journal of Surgical Oncology, 123(6), pp. 1447–1458.
- Davis, A.M. et al. (2016) ‘Radiation therapy for primary bone sarcoma: a systematic review’, Radiotherapy and Oncology, 119(3), pp. 409–417.
- Czarnecki, J.S. et al. (2015) ‘Molecular pathogenesis of osteosarcoma’, Journal of the National Cancer Institute, 107(11), djv234.
- Tsuchiya, H. et al. (2005) ‘Function and oncologic outcome after rotationplasty for lower-limb sarcomas’, Clinical Orthopaedics and Related Research, 436, pp. 210–217.
- Ferrari, S. et al. (2010) ‘Prognostic factors in non-metastatic osteosarcoma of the extremities: a study of 250 patients treated at the Rizzoli Institute’, Journal of Orthopaedic Science, 15(5), pp. 616–623.
- Gangi, A. et al. (2019) ‘Imaging of osteosarcoma: current diagnostic approach and update’, European Radiology, 29(11), pp. 6028–6040.