

What is Melanoma?
Your skin is the largest organ in your body, and it does a heavy job protecting you from the environment. Deep inside the top layer of your skin (the epidermis), there are special cells called melanocytes. These cells produce a pigment called melanin, which gives your skin its color. When you go out in the sun, these cells make more melanin to try and protect you, which creates a tan.
Melanoma happens when these color-producing cells start growing out of control. It is a type of skin cancer. While it is not the most common type of skin cancer (Basal Cell and Squamous Cell cancers are more common), melanoma is considered the most dangerous. This is because it is more likely to spread (metastasize) to other parts of the body if it is not caught early [1].
However, there is good news. When melanoma is found early—before it spreads deep into the skin or to other organs—it is highly curable. This guide will help you understand what to look for, how doctors find it, and what treatments are available, all based on trusted medical data.

Early signs of Melanoma: Symptoms Table
Melanoma can appear anywhere on the body. In men, it often shows up on the chest or back. It commonly appears on the legs in women. However, it can also hide in places you might not expect, like between your toes, under a fingernail, or even in your eyes [2].
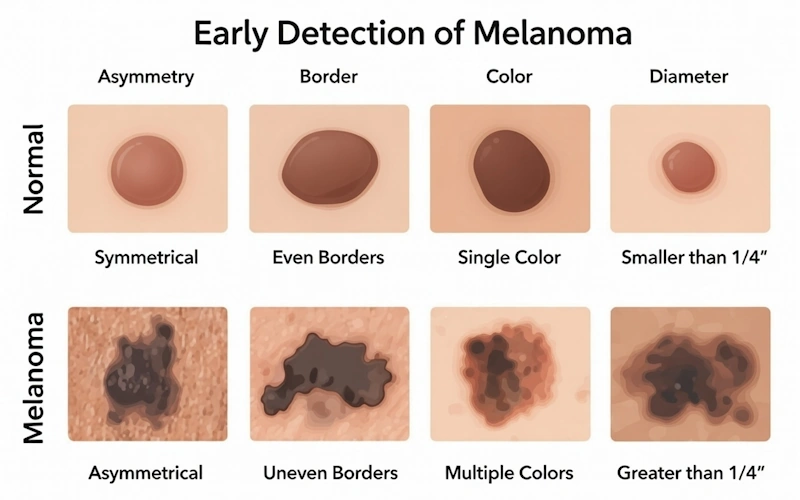
The primary indicator of melanoma is a shift in an existing mole or the emergence of a new growth with atypical features. Doctors use the ABCDE rule to help people identify potential warning signs.
| Symptom (ABCDE) | Real-Life Feel | When to Worry |
| A: Asymmetry | Imagine folding the mole in half. If the two halves do not look the same, that is asymmetry. | If one half is round and the other half is jagged or a different shape. |
| B: Border | A normal mole has a smooth, even edge. A cancerous mole often has a blurry, rough, or “ragged” edge. | If the edges look like a map of a coastline rather than a perfect circle. |
| C: Color | Most normal moles are one solid color (usually brown). Melanomas often have mixed colors. | Look for shades of tan, brown, and black mixed together. Sometimes you might see white, red, or blue. |
| D: Diameter | This parameter explains the size of the inspected mole. | If the spot is larger than a pencil eraser (about 6 millimeters), get it checked. However, some melanomas start smaller. |
| E: Evolving | “Evolving” means changing. This is the most important sign. | If a mole starts itching, bleeding, crusting, or changing size/shape/color over a few weeks or months. |
The “Ugly Duckling” Sign
Another easy way to spot a problem is the “Ugly Duckling” sign. Most of your moles probably look similar to one another—like a family. If you have one mole that stands out and looks completely different from all the others on your body, that is the “Ugly Duckling.” It should be checked by a doctor immediately [1, 2].
 Sergey Prikhodko, oncologist, PhD: “The human brain is actually quite poor at remembering exactly how a spot looked three months ago. I always advise my patients to use their phones. If you are ‘on the fence’ about a mole, take a picture of it next to a reference object, like a coin or a ruler. Repeat this once a month. If the photos show growth or change, you have concrete proof to show your dermatologist.”
Sergey Prikhodko, oncologist, PhD: “The human brain is actually quite poor at remembering exactly how a spot looked three months ago. I always advise my patients to use their phones. If you are ‘on the fence’ about a mole, take a picture of it next to a reference object, like a coin or a ruler. Repeat this once a month. If the photos show growth or change, you have concrete proof to show your dermatologist.”
Root Causes of Melanoma (Risk Factors + Genetic Links)
You might be wondering, “Why did this happen?” or “Am I at risk?” Scientists and doctors have identified several factors that increase the chance of developing melanoma. It is usually a combination of your environment and your DNA.
1. Ultraviolet (UV) Light
UV exposure represents the leading trigger for the majority of skin cancers, as it damages DNA in skin cells.
- The Sun: Natural sunlight contains UV rays. Severe, blistering sunburns (especially when you are a child or teenager) significantly increase your risk later in life.
Tanning Beds: Artificial UV light is just as dangerous, if not more so. Using tanning beds increases the risk of melanoma, especially if you start using them before age 30 [1, 3].
Sergey Prikhodko, oncologist, PhD: “There is a dangerous myth that getting a ‘base tan’ prevents sunburn and protects you. This is scientifically false. A tan is actually your skin’s injury response—it means DNA damage has already occurred. Seeking a base tan is essentially pre-damaging your skin before you even go on vacation.”
2. Genetics and Family History
Your genes play a major role in your skin’s ability to protect itself.
- Fair Skin: People with fair skin, light hair (blonde or red), and light eyes (blue or green) have less melanin. Melanin provides inherent defense from UV radiation. Without it, the skin burns easily, leading to DNA damage [4].
- Family History: If your parents or siblings have had melanoma, your risk is higher. About 8% of people with melanoma have a first-degree relative who also had it [4].
- Gene Mutations: Specific gene changes can run in families. For example, changes in the CDKN2A gene can stop the body from controlling cell growth properly. Another gene, MC1R, is responsible for red hair and fair skin; mutations here make the skin more sensitive to the sun [4].
3. Moles (Nevi)
Having a lot of moles (more than 50) puts you at higher risk. Also, having “dysplastic nevi” (moles that look unusual but aren’t cancer yet) increases risk. These moles are often larger than average and have irregular shapes [2].
4. Weakened Immune System
People who take medicines that suppress the immune system (for example, after an organ transplant) or people with conditions like HIV/AIDS have a harder time fighting off cancer cells, including melanoma [1].
Diagnosis of Melanoma: Tests Explained
If you find a suspicious spot, your first step is to see a doctor. They will look at your skin, but they cannot tell for sure if it is cancer just by looking. They need to do tests.
Visual Exam
The doctor will ask if the mole has changed recently. To inspect the mole, doctor often uses a medical tool called a dermatoscope. This is a special magnifying glass with a light that allows them to see pigment patterns deep in the skin that the naked eye cannot see [2].

Skin Biopsy
If the doctor thinks a spot looks dangerous, they will remove part or all of it to test it in a lab. This is called a biopsy.
- Punch Biopsy: The doctor uses a circular tool (like a tiny cookie cutter) to remove a round piece of skin.
- Excisional Biopsy: The doctor uses a scalpel to remove the entire mole and a small border of normal skin around it. This is often preferred for melanoma to see how deep it has grown.
- Shave Biopsy: The doctor shaves off the top layer of skin. This is less common for suspected melanoma because it might not go deep enough to measure the cancer’s thickness [1, 2].
Sergey Prikhodko, oncologist, PhD: “Patients often get nervous when they hear the word ‘biopsy,’ but it is important to know that a skin biopsy is usually a very quick, in-office procedure performed under local anesthesia. It typically takes less than ten minutes, and most patients report feeling nothing more than a tiny pinch. It is a small moment of discomfort for a massive amount of peace of mind.”Staging
If the lab confirms melanoma, the doctor needs to know the “Stage.” The stage tells you how thick the tumor is and if it has spread.
- Stage 0 (Melanoma in Situ): The cancer is only in the very top layer of skin. It has not grown inward.
- Stage I and II: The cancer is in the skin but has not spread to lymph nodes. Thicker tumors are higher stages.
- Stage III: The cancer has spread to nearby lymph nodes or skin vessels.
- Stage IV: The cancer has spread to distant organs like the lungs, liver, brain, or bones [2].
To find the stage, doctors might do a Sentinel Lymph Node Biopsy. They inject a dye near the tumor to see which lymph node the fluid drains to first. They remove that node and check it for cancer cells.
Melanoma Treatment
Treatment depends entirely on the stage of the cancer and your overall health. Here is a simplified roadmap of how doctors typically treat melanoma.
| Step | How-To | Tips |
| 1. Surgery | This is the main treatment for early-stage melanoma. The doctor cuts out the tumor and a margin of healthy safety skin around it (Wide Local Excision). | For very thin melanomas, this might be the only treatment you need. You will have a scar, but you will be cancer-free. |
| 2. Lymph Node Removal | If the cancer has spread to the lymph nodes (Stage III), the surgeon may remove the affected nodes (Lymphadenectomy). | This can sometimes cause swelling in the arm or leg (lymphedema). Ask your doctor about physical therapy to manage this. |
| 3. Immunotherapy | These drugs help your own immune system recognize and attack cancer cells. Examples include Pembrolizumab (Keytruda) or Nivolumab (Opdivo). | These are often used for Stage III or IV melanoma. They are given through an IV (vein). Side effects can feel like the flu. |
| 4. Targeted Therapy | If your melanoma has a specific gene mutation (like BRAF), doctors can prescribe pills that target that specific mutation to shrink the tumor. | About half of melanomas have a BRAF mutation. Your doctor will test your tumor DNA to see if these drugs will work for you. |
| 5. Radiation Therapy | High-energy beams (like strong X-rays) are used to kill cancer cells. | This is usually used if surgery isn’t an option, or to treat melanoma that has spread to the brain or bones to relieve pain. |
| 6. Chemotherapy | Traditional cancer drugs that kill fast-growing cells. | This is used much less often now because Immunotherapy and Targeted Therapy usually work better for melanoma. |
Daily Tips for Melanoma Prevention
Whether you have had melanoma or just want to prevent it, protecting your skin is a lifelong commitment. You do not have to stay indoors forever, but you do need to be smart about the sun.
- Master the Sunscreen: Use a “Broad Spectrum” sunscreen. This protects against both UVA (aging) and UVB (burning) rays.
- Use SPF 30 or higher.
- Apply it 15 minutes before you go outside.
- Reapply every 2 hours, or immediately after swimming or sweating. Water-resistant does not mean waterproof!
- Clothing is Key: Wearing a shirt is better than sunscreen. Look for clothing with an UPF (Ultraviolet Protection Factor) label. Wear a hat with a wide brim to protect your ears and neck (a baseball cap leaves your ears exposed) [1].
- Seek Shade: The sun is strongest between 10:00 AM and 4:00 PM. If your shadow is shorter than you are, the sun is dangerous. Stay under a tree or umbrella during these hours.
- Avoid Tanning Beds Completely: There is no such thing as a “safe base tan.” Tanning beds pump concentrated UV rays directly into your skin. Use spray tans or lotions if you want color.
- Perform Monthly Self-Exams:
- Stand in front of a full-length mirror.
- Check your front, back, and sides.
- Raise your arms and check your underarms.
- Look at your forearms, palms, and under your fingernails.
- Sit down and check your legs, feet, soles, and between your toes.
- Use a hand mirror to check the back of your neck and your scalp (part your hair).
Sergey Prikhodko, oncologist, PhD: “The number one failure point I see with sunscreen isn’t that people forget to wear it—it’s that they don’t wear enough of it. To get the SPF number listed on the bottle, you need to apply about a full shot glass (one ounce) of lotion to your body. If you are using a spray, if your skin doesn’t glisten or look wet before you rub it in, you haven’t used enough.”How is life affected by melanoma?
For most people who have had melanoma, there are no physical or practical obstacles to continuing with life as it was before the diagnosis. Nevertheless, it is common for life to change. You always carry the experiences of what you have been through with you.
It can feel difficult at times. Most people think it gets better, even if it may take time. Some feel vulnerable and anxious long after treatment is over. Here you can read about help with thoughts and feelings in cancer.
You may experience swelling in an arm or leg if the surgeon had to remove all the lymph nodes in, for example, an armpit or groin. This is called lymphedema. Help is available.
Treatment may need to be followed up
It varies from person to person whether treatment needs to be followed up, and how much follow-up is needed. It depends on the risk that the cancer will come back or spread.
There is little risk of getting sick again if the cancer was detected early. The risk also decreases the longer it has been since treatment ended.
A follow-up involves the doctor examining the scar, the skin around the scar, and the lymph nodes.
Melanoma vs. Basal Cell Carcinoma: Quick Compare
It is easy to get confused between different skin cancers. Here is how to tell the difference between the two most discussed types.
| Feature | Melanoma | Basal Cell Carcinoma (BCC) |
| Appearance | Usually dark brown, black, or mixed colors. Irregular borders. | Often looks like a pearly or waxy bump. It may present as a flat, scar-like lesion that is flesh-colored or brown. |
| Speed of Growth | Can grow and change quickly (weeks to months). | Usually grows very slowly (over years). |
| Danger Level | High. Can spread (metastasize) to other organs and be fatal if untreated. | Low. This type of cancer almost never spreads. |
| Common Location | Chest, back, legs, but can be anywhere. | Sun-exposed areas: Face, ears, neck, scalp, shoulders. |
| Treatment | Surgery, often followed by medicine (immunotherapy) if it spreads. | Surgery (Mohs surgery) is usually curative. |
(Source: MedlinePlus – Melanoma [1]; MedlinePlus – Basal Cell Carcinoma [3])
FAQs
Q: Is melanoma always caused by the sun?
A: Not always. While UV light is the biggest risk factor, melanoma can appear in places the sun never shines, like the soles of your feet, inside your mouth, or on your genitals. This suggests that genetics and other factors also play a big role [2, 4].
Q: Can a mole turn into melanoma if I scratch it or cut it?
A: No. Injuring a mole does not cause cancer. However, if a mole bleeds easily on its own without you scratching it, that is a warning sign that it might already be cancerous. You should get it checked [2].
Q: Does melanoma run in families?
A: It can. About 1 in 10 patients with melanoma has a family member who also had it. If you have a strong family history, your doctor might recommend more frequent skin checks or genetic counseling [4].
Q: Is melanoma itchy?
A: Sometimes. While many melanomas are painless, some people report that the spot feels itchy, tender, or painful. If a mole starts to itch and doesn’t stop, show it to a doctor [1].
Q: If I have dark skin, can I still get melanoma?
A: Yes. People with darker skin naturally have more protection against the sun, so their risk is lower than people with fair skin. However, when people with dark skin do get melanoma, it is often found at a later, more dangerous stage. It frequently appears in non-sun-exposed areas like the palms of the hands or soles of the feet (acral lentiginous melanoma) [1].
Sergey Prikhodko, oncologist, PhD: “This is a critical point. Because patients with darker skin tones (like Bob Marley, who famously passed away from acral melanoma) often believe they are immune to skin cancer, they tend to be diagnosed at much later stages. Regardless of your skin tone, check your palms, soles, and nail beds regularly. Pigmentation does not equal immunity.”Sources & References
- MedlinePlus [Internet]. Bethesda (MD): National Library of Medicine (US); [updated 2025 Oct 25]. Melanoma; [cited 2025 Nov 1]. Available from: https://medlineplus.gov/melanoma.html
- MedlinePlus Medical Encyclopedia [Internet]. Bethesda (MD): National Library of Medicine (US); [updated 2025 Oct 25]. Melanoma; [cited 2025 Nov 1]. Available from: https://medlineplus.gov/ency/article/000850.htm
- MedlinePlus [Internet]. Bethesda (MD): National Library of Medicine (US); [updated 2025 Oct 25]. Basal Cell Carcinoma; [cited 2025 Nov 1].
- MedlinePlus: Genetics [Internet]. Bethesda (MD): National Library of Medicine (US); [updated 2025 Oct 01]. Melanoma; [cited 2025 Nov 1]. Available from: https://medlineplus.gov/genetics/condition/melanoma/